

Facial Nerve Rehabilitation
Can removal of an acoustic neuroma affect the facial nerve?
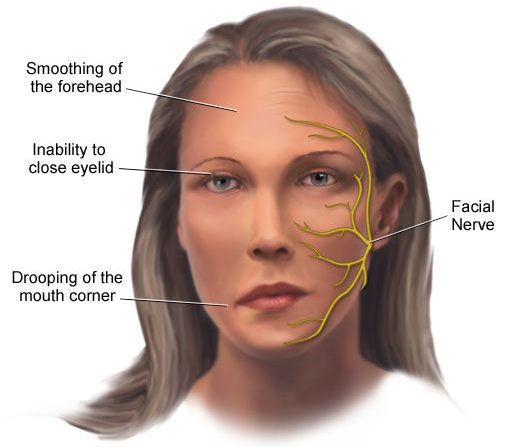
Acoustic neuromas are in close contact with facial nerves which are responsible for the muscles of facial expression and for closing the eyes. Temporary facial paralysis may occur after acoustic neuroma resection, and weakness may persist for 6 to 12 months. Few patients have permanent facial weakness. Facial paralysis can result from swelling or nerve damage. Swelling is common because the nerve is compressed and distorted by the tumor in the internal auditory canal.
What can be done for rehabilitation?
Careful tumor removal using an operating microscope and monitoring of the facial nerve often results in its preservation. Stretching of the facial nerve can also result in swelling with subsequent temporary facial paralysis. In these cases, facial nerve function is closely monitored for months after the procedure. If it is certain that facial nerve function will not recover over time (1-2% of cases), a second surgery can be performed to connect the facial nerve with a nerve in the neck (hypoglossal-facial anastomosis).
In 1-2% of cases the facial nerve passes through the middle of the acoustic neuroma. In addition, the tumor may originate in the facial nerve itself (facial neuroma). In these situations, it is necessary to remove part or all of the nerve for tumor resection. When this is needed, the facial nerve can be immediately reconnected or a nerve “bridge” can be performed with a nerve of the neck to provide sensation.
When it is not possible to reconnect or “bridge” the facial nerve, a second surgery may be performed to reanimate the face. One option is hypoglossal-facial anastomosis, connecting the nerve of the tongue with the nerve of the face. Another option is facial resuscitation surgery in which the temporal (mastication) muscle is connected to the muscles of the face to aid in movement.